Introduction
Glaucoma is a progressive optic neuropathy – damage to the optic nerve and retinal nerve fibers – that slowly steals vision. It is now the world’s second-leading cause of blindness (pmc.ncbi.nlm.nih.gov). Rather than causing blunt vision loss like cataracts, glaucoma typically creates blind spots (called scotomas) and patches of reduced sensitivity in the visual field. Depending on the eye and disease type, these scotomas can look very different. Some glaucoma patients see large regional areas of vision loss (for example, an arc-shaped “slice” or nasal wedge of blindness), while others only have numerous small “peppered” defects scattered across their field. Understanding these patterns helps patients interpret test results and helps doctors predict how the disease may behave. This article will explain why glaucoma produces large blind spots in some cases versus diffuse scattered losses in others, what this means for different glaucoma subtypes and progression, and how these patterns affect daily life, treatment, and monitoring (pmc.ncbi.nlm.nih.gov) (www.nature.com).
How Glaucoma Causes Visual Field Loss
Inside the eye, the retinal ganglion cells send visual information along axons (the retinal nerve fiber layer) to form the optic nerve. In glaucoma, these nerve fibers die off. Because the fibers are organized into bundles (arcuate bundles that arc above and below the blind spot at the optic nerve head), damage tends to follow predictable paths (pmc.ncbi.nlm.nih.gov). For example, an arcuate scotoma follows the path of fibers over the macula, forming an arc-shaped blind region from the blind spot into peripheral field. A nasal step defect appears as an abrupt loss across the horizontal midline into the nasal (inner) field. In contrast, a generalized or diffuse defect involves a more uniform loss of sensitivity across many retinal locations rather than one localized patch (pmc.ncbi.nlm.nih.gov) (www.nature.com). In a normal visual field test, each eye has a “blind spot” (where the optic nerve exits the retina) about 15° to the side of central fixation (pmc.ncbi.nlm.nih.gov). Glaucoma adds to this natural blind spot by progressively enlarging it or creating new blind regions elsewhere in the field.
Common Patterns of Visual Field Loss
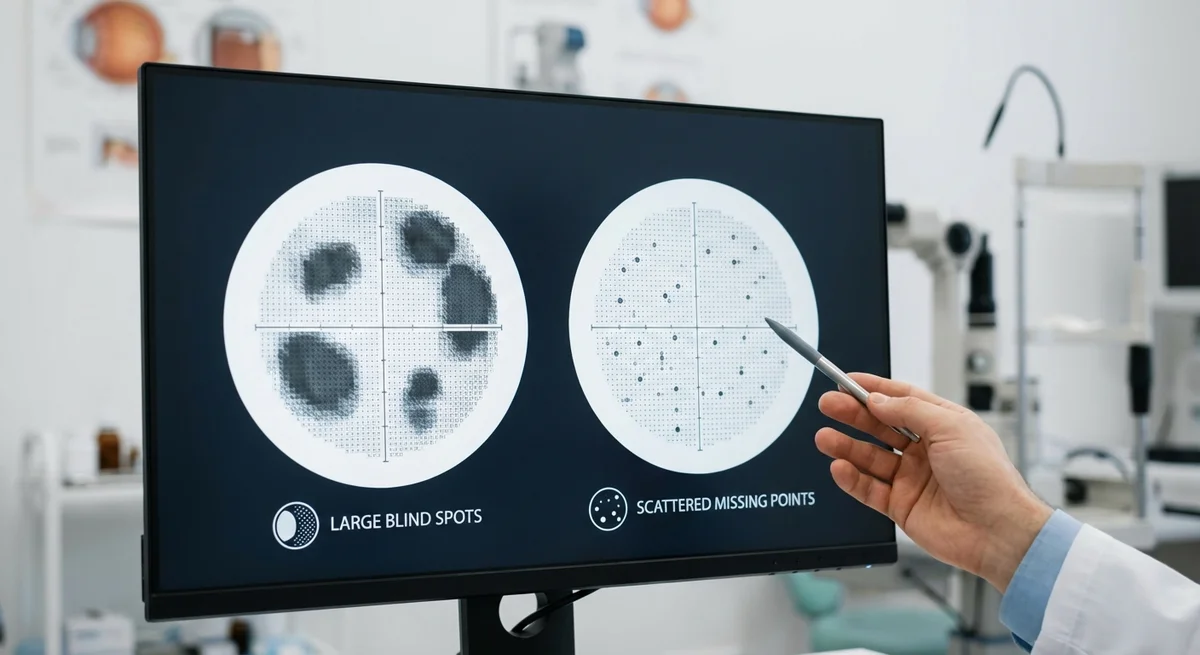
Glaucoma visual field loss can broadly be categorized into localized (contiguous) defects and diffuse/scattered defects.
-
Localized defects (large scotomas) – These are relatively large, continuous areas of vision loss that often align with nerve-fiber anatomy. Classic examples include arcuate scotomas (curving from the blind spot toward the nasal field), paracentral scotomas (small defects just next to fixation), nasal steps (a visible step-like loss at the horizontal meridian), and altitudinal defects (loss of an entire upper or lower half of vision). In fact, early glaucoma often produces arcuate or paracentral scotomas and nasal steps along the midline (pmc.ncbi.nlm.nih.gov). For example, one review reported that among patients with primary open-angle glaucoma (POAG), the nasal step was the most frequent early defect, followed by paracentral and arcuate scotomas (pmc.ncbi.nlm.nih.gov). These localized defects respect the anatomy of nerve fiber bundles and typically spare other regions until the disease advances (pmc.ncbi.nlm.nih.gov) (www.nature.com).
-
Diffuse or scattered defects (small-point losses) – Other patients show many isolated points of sensitivity loss scattered across the field, often without a coherent large pattern. These may appear as scattered “peppery” dots where a few retinal test points register lower sensitivity. This can indicate a mild, generalized loss of retinal function without a full-blown blind area. Research shows that a component of diffuse sensitivity decrease often exists at all stages of glaucoma (www.nature.com). In fact, early in glaucoma a modest diffuse depression may be measured, which over time coalesces into larger pattern defects (www.nature.com). Only when many small defects deepen and merge do they form the more obvious broad scotomas. It’s worth noting that true diffuse loss is relatively uncommon in early glaucoma (often what looks like diffuse loss is due to cataract or poor test conditions) (pmc.ncbi.nlm.nih.gov) (www.nature.com). When doctors see many small scattered points of loss but no clear shape, they consider whether other factors (like media opacity or test reliability) might be contributing (pmc.ncbi.nlm.nih.gov).
Thus, large blind spots result from contiguous nerve-fiber bundle damage (often seen in more advanced or high-pressure glaucoma), whereas scattered missing points often reflect an earlier or milder stage of loss, or a widespread slight reduction in sensitivity (www.nature.com) (pmc.ncbi.nlm.nih.gov). Importantly, a series of small defects can be an early warning – as glaucoma progresses, these tend to grow together into larger scotomas (www.nature.com).
Why Do Patterns Differ? Factors Behind the Shape of Loss
Several factors influence whether glaucoma produces large scotomas versus scattered points of loss.
Stage of Disease
The amount of damage (how many retinal cells are lost) strongly affects the pattern. In early glaucoma, many small areas of nerve-fiber damage may surround warning signs of glaucoma, causing a more diffuse, patchy appearance on the visual field. As damage deepens in those areas, the small points of loss merge into one large defect. Studies have found exactly this evolution: “early diffuse field loss converts into well-defined pattern defects at later stages” (www.nature.com). In other words, a patient whose visual field shows a mild scattered depression now may later develop a large scotoma in that region as glaucoma progresses.
Conversely, if someone already has advanced glaucoma, the test will show large continuous zones of no vision. In very late disease, only a thin strip of vision near fixation or the nasal field remains. Clinicians therefore interpret a very large or connected scotoma as a sign of advanced damage, whereas scattered single-point deficits suggest earlier or slow damage progression (www.nature.com) (pmc.ncbi.nlm.nih.gov).
Glaucoma Subtype and Risk Factors
Different glaucoma subtypes and risk factors tend to produce different patterns of loss. Primary open-angle glaucoma (POAG) includes both high- and normal-tension forms, and angle-closure glaucoma (PACG) is another type. Research suggests some tendencies:
-
**Normal-Tension Glaucoma (NTG)**. In NTG, eye pressure is in the normal range, and vascular factors are thought to play a larger role. NTG often targets the deeper bundles near the center of vision. Several studies report that NTG patients more frequently have central or paracentral scotomas, defects that are dense and close to fixation (pmc.ncbi.nlm.nih.gov) (pmc.ncbi.nlm.nih.gov). For example, one analysis noted NTG tends to cause “deeper, more central, and more depressed” visual field loss than high-pressure glaucoma (pmc.ncbi.nlm.nih.gov). Another found that initial paracentral scotomas in NTG progressed inward toward fixation over time (www.nature.com). These central losses may relate to NTG-associated blood-flow or vascular issues (pmc.ncbi.nlm.nih.gov) (www.nature.com).
-
High-Tension Glaucoma (HTG) and POAG. In contrast, POAG with higher pressures (or younger patients) more often produces the classic wide arcuate and nasal-step defects along the periphery of the central field (pmc.ncbi.nlm.nih.gov) (pmc.ncbi.nlm.nih.gov). A study comparing HTG to NTG found that nasal steps and arcuate scotomas tended to be deeper in HTG (pmc.ncbi.nlm.nih.gov). In general, POAG patients might show a more diffuse loss earlier, whereas NTG shows more localized dense losses (pmc.ncbi.nlm.nih.gov) (pmc.ncbi.nlm.nih.gov). However, not all research agrees: some studies found few differences between NTG and HTG field patterns (pmc.ncbi.nlm.nih.gov) (pmc.ncbi.nlm.nih.gov).
-
**Angle-Closure Glaucoma (PACG)**. Patients with angle-closure glaucoma often have worse overall field loss. One large study found that angle-closure cases had more severe loss (lower mean deviations) than open-angle cases, and their topography was slightly different: POAG eyes tended to have more upper (superior) field loss, whereas PACG eyes were more evenly affected top vs. bottom (jamanetwork.com). In practical terms, clinicians note that PACG can damage both upper and lower fields, possibly leading to wider scotomas, while POAG often starts in the upper field near the blind spot (jamanetwork.com) (pmc.ncbi.nlm.nih.gov).
-
Other factors. Age, race, and genetic differences may also shape patterns, although specifics are less clear. Cataracts or small pupils can simulate diffuse loss across the field (pmc.ncbi.nlm.nih.gov), so doctors must rule out those factors. Vascular health (blood pressure, perfusion) especially affects NTG patterns (pmc.ncbi.nlm.nih.gov) (www.nature.com). Details of the optic nerve anatomy (disc size, nerve fiber layer thickness) can predispose one area to fail first.
In summary, glaucoma subtype and underlying disease mechanism influence pattern: NTG (and related vascular risk) generally causes small central losses, while high-pressure POAG causes more peripheral arcuate scotomas (pmc.ncbi.nlm.nih.gov) (www.nature.com). Over time, the current pattern will worsen along those characteristic zones.
Impact on Daily Life and Quality of Life
The pattern of field loss has real consequences for function. Central vs peripheral deficits affect different tasks:
-
Central scotomas (near fixation) severely impact tasks like reading, recognizing faces, and detailed work. For instance, an absolute blind area within 3° of fixation (right around where we focus) can noticeably slow reading speed and make text hard to decipher (pubmed.ncbi.nlm.nih.gov). In fact, one study found that only patients whose central scotomas covered more than 2 adjacent quadrants had subjective reading difficulty (pubmed.ncbi.nlm.nih.gov). Another review emphasizes that even small central defects make driving and other tasks much harder (pmc.ncbi.nlm.nih.gov).
-
Peripheral or large arcuate defects more strongly affect mobility and orientation. Losing a chunk of side vision (for example, a large nasal step or an inferior altitudinal defect) can impair ability to see obstacles or moving objects at the edges. Patients often report bumping into things or trouble walking comfortably. This difficulty is borne out in studies: people with significant peripheral loss take shorter strides and have more variability when walking, reflecting difficulty in spatial awareness (pubmed.ncbi.nlm.nih.gov).
One systematic review found that both central and peripheral visual field loss greatly hinders driving skills and daily activities (pmc.ncbi.nlm.nih.gov) (pmc.ncbi.nlm.nih.gov). In fact, central field defects caused more driving problems than peripheral ones (pmc.ncbi.nlm.nih.gov), because obstacles directly ahead are crucial for safe driving. Another study showed that overall quality of life was similarly reduced by glaucoma (a peripheral loss disease) as by macular degeneration (a central loss disease), although glaucoma patients tended to experience more emotional or social impact than physical limitations (pmc.ncbi.nlm.nih.gov). In practice, patients with any noticeable scotomas – whether a big patch or a cluster of smaller holes – often develop coping strategies (such as moving their eyes slightly to scan with healthy areas) but still face challenges.
In short, large blind spots (especially if they encroach near the center or cover much of a quadrant) tend to produce obvious functional losses (like difficulty reading or moving safely), whereas scattered points may go unnoticed individually but cumulatively can reduce contrast sensitivity and make the visual world seem “grainy.” Both types of loss can reduce independence: climbing stairs and walking around outside become harder (pmc.ncbi.nlm.nih.gov), and standard activities like driving, working, and even navigating familiar environments can be compromised.
Treatment Response and Monitoring Implications
Treatment for glaucoma always focuses on slowing damage, mainly by lowering intraocular pressure (IOP) or addressing underlying risk factors. Generally, the medical or surgical treatment does not change simply because of the pattern of loss. Both a broad arcuate scotoma and scattered small losses warrant aggressive control of glaucoma risk factors. However, clinicians often note patterns to guide monitoring: for example, a new paracentral scotoma (near fixation) usually prompts closer follow-up, because it threatens critical vision (www.nature.com). Specialized testing (such as a 10-2 visual field) may be used to monitor small central areas more closely if paracentral defects appear.
As of now, there is no specific medication that “fixes” one pattern versus another. Instead, patterns mainly influence prognosis and vigilance. A large arcuate defect usually indicates more extensive nerve damage, suggesting the disease is advanced and may have progressed significantly already. In contrast, many small scattered spots might indicate early or slowly progressive disease. Some studies suggest particular patterns in early disease herald faster progression: for instance, initial paracentral scotomas (especially in NTG) were linked to deeper future loss and vascular risk factors (www.nature.com). Also, large prospective trials have shown that eye regions corresponding to those early arcuate defects tend to worsen first if glaucoma is unchecked (pmc.ncbi.nlm.nih.gov). These findings imply that if a patient has a detectable nasal step or paracentral scotoma, doctors should treat and monitor aggressively, paying special attention to those “vulnerable” zones (pmc.ncbi.nlm.nih.gov) (www.nature.com).
In practice, that means regular follow-up visual field testing focusing on the areas where loss has appeared. An initial scattered pattern of points might simply be watched over time to see if it deepens into a larger scotoma. Conversely, seeing a large scotoma appear (for example, an arcuate defect) often leads to verifying that it was a reliable finding and possibly doing more visual field tests to check stability. Optical coherence tomography (OCT) scans of the nerve fiber layer can complement field findings to see if structure matches function.
Conclusion
In summary, glaucoma can create both broad visual field defects and diffuse dotted losses, and understanding the difference is important for patients and doctors. Large contiguous scotomas (for example, arcuate or nasal-step defects) reflect significant nerve-fiber bundle damage along known anatomical paths. Scattered small-point defects often signal a milder, diffuse sensitivity loss that may precede the formation of a larger blind spot. Several factors influence these patterns: glaucoma subtype (NTG vs POAG vs PACG), stage of disease, and possibly the underlying cause of nerve damage (vascular vs pressure). Importantly, these patterns have practical implications. Big scotomas can drastically affect vision-related tasks (reading, climbing stairs, driving), while scattered points degrade overall visual capacity and mobility in subtler ways (pmc.ncbi.nlm.nih.gov) (pubmed.ncbi.nlm.nih.gov).
For patients, recognizing whether their test shows a patch of lost vision or many tiny deficits can guide expectations. For clinicians, it helps tailor monitoring – for example, new central or nasal losses often trigger closer scrutiny (pmc.ncbi.nlm.nih.gov) (www.nature.com). Ultimately, regardless of pattern, the goal is the same: preserve as much vision as possible. Keeping IOP low and retinal nerve fibers healthy is key, whether the field resembles Swiss cheese or has a few large holes. By correlating patterns of field loss with disease type and progression in each patient, doctors can better predict how glaucoma will evolve. Patients, for their part, can use this understanding to make sense of their visual field results and to stay informed partners in their care.