Carotid-Cavernous Fistulas and Eye Pressure
Carotid-cavernous fistulas (CCFs) are abnormal connections between an artery and the venous cavernous sinus at the base of the skull. In simple terms, blood that should flow through arteries is shunted directly into veins. This raises the blood pressure inside the eye’s venous system. The extra pressure backs up into the veins around the eye, raising the episcleral venous pressure (the pressure in veins near the surface of the eyeball). When this happens, the eye’s fluid outflow is blocked, and intraocular pressure (IOP) rises, potentially causing secondary glaucoma (pmc.ncbi.nlm.nih.gov) (pubmed.ncbi.nlm.nih.gov).
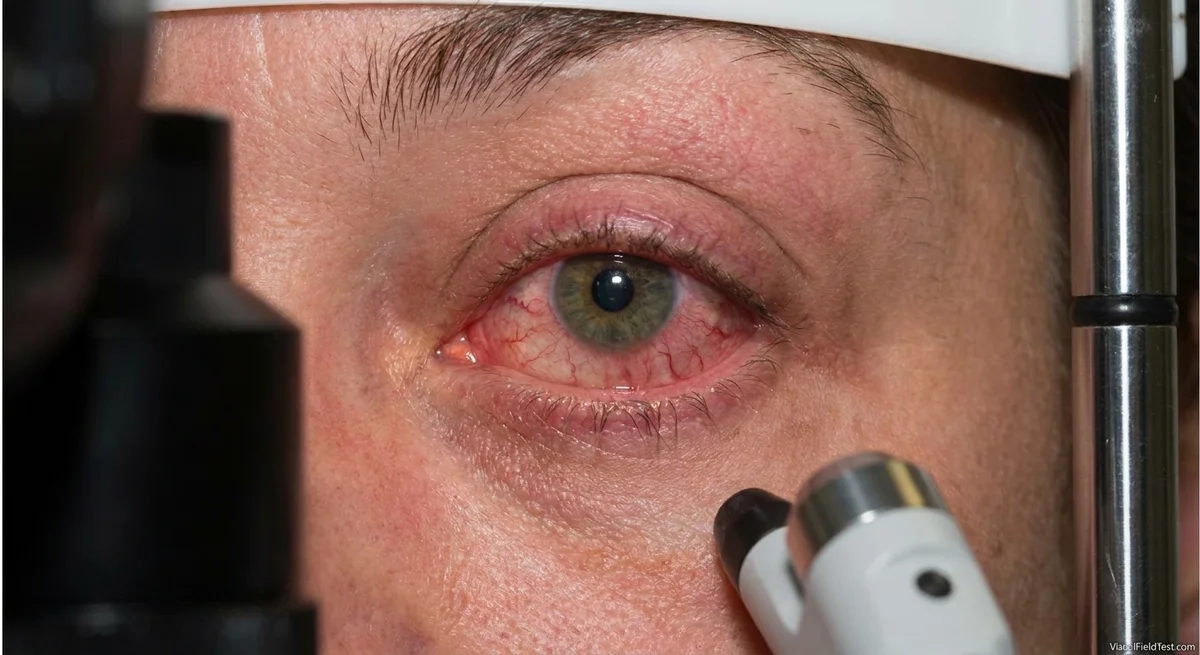
Early signs of a CCF can include a red, swollen eye, a bulging eyeball (proptosis), a noise like a whoosh in the head (bruit), and vision changes. These findings result from venous hypertension – high pressure in the eye’s veins. Because of the slow, high-pressure blood flow, the normally thin conjunctival veins become “arterialized” (bright red and corkscrew-shaped). Patients may also have chemosis (conjunctival swelling) and double vision if eye-movement nerves are affected. Knowing these symptoms helps prompt imaging and treatment, which can quickly lower eye pressure and protect vision (pmc.ncbi.nlm.nih.gov) (pmc.ncbi.nlm.nih.gov).
How CCFs Raise Eye Pressure
There are two main types of carotid-cavernous fistulas, and both create orbital venous hypertension. Direct CCFs (Barrow type A) occur when the main internal carotid artery tears directly into the cavernous sinus. This usually happens in trauma (head injury or skull fracture), or rarely from a ruptured aneurysm. Because the tear is large, these fistulas are high-flow. A huge wave of arterial blood rushes into the venous cavernous sinus and then retrogrades (flows backward) into the eye’s veins. Indirect or dural CCFs (types B, C, D) involve small meningeal branches of the carotid or external carotid arteries feeding the sinus. These connections are smaller and low-flow, often developing spontaneously in older adults. Even though dural CCFs are lower flow, they still raise sinus pressure over time (pmc.ncbi.nlm.nih.gov) (pmc.ncbi.nlm.nih.gov).
In both cases, the key is that arterial blood at high pressure enters the cavernous sinus, crowding out normal venous flow. This creates venous stasis and back-pressure. The superior ophthalmic vein (and sometimes inferior ophthalmic vein) carries blood from the eye to the cavernous sinus. When the cavernous sinus pressure climbs above the pressure in those veins, flow reverses or stalls (pmc.ncbi.nlm.nih.gov). These veins become engorged, and the normal balance of fluid in the eye is disturbed. The eye constantly produces watery fluid (aqueous humor), and normally this drains out through veins. If the veins are jammed by high pressure, the fluid cannot drain, and the eye pressure rises to match the venous pressure (link.springer.com) (pmc.ncbi.nlm.nih.gov).
The normal episcleral venous pressure is only about 8–10 mmHg (link.springer.com). In a CCF, that pressure can jump much higher. Once the episcleral pressure reaches the level of the IOP, any further increase in venous pressure forces the IOP to rise almost equally (link.springer.com). In practical terms, every extra mmHg of pressure in the eye’s veins directly adds to the eye’s internal pressure. As a result, patients with CCF often develop a secondary open-angle glaucoma where fluid cannot exit because of the high back-pressure (pmc.ncbi.nlm.nih.gov) (link.springer.com).
(Note: In rare cases, the raised pressure can also push the iris forward, shallowing the front chamber and causing angle-closure glaucoma, or cause poor retinal blood flow and new troublesome vessels. But most CCF-related glaucoma is from the simple effect of blocked venous outflow (pmc.ncbi.nlm.nih.gov) (link.springer.com).)
Recognizing the Key Eye Findings
When a carotid-cavernous fistula develops, it often creates striking eye signs. One of the hallmarks is arterialized conjunctival vessels. Normally the white of the eye has fine red veins. In CCF, those veins look bright red, engorged, and tortuous (often described as “corkscrew” vessels) because they carry direct arterial blood (pmc.ncbi.nlm.nih.gov) (pmc.ncbi.nlm.nih.gov). Patients usually have conjunctival chemosis – swelling of the clear membrane (conjunctiva) covering the white of the eye – causing a bloodshot, puffy appearance (pmc.ncbi.nlm.nih.gov) (pmc.ncbi.nlm.nih.gov).
Another classic feature is proptosis (bulging of the eyeball). Because the venous congestion extends behind the eye, the eye can protrude forward, and in a high-flow fistula it may even pulsate in time with the heartbeat (pmc.ncbi.nlm.nih.gov) (pmc.ncbi.nlm.nih.gov). Eye movement can become limited too, and patients often develop double vision (diplopia) if the cranial nerves or engorged eye muscles are affected. There may also be ptosis (drooping eyelid) or an enlarged pupil on that side if the nerves in the sinus are involved.
A very important clue is the orbital bruit. This is an abnormal whooshing or throbbing sound heard by placing a stethoscope over the eye or temple. High-flow fistulas typically create an audible bruit synchronous with the heartbeat; even low-flow fistulas can sometimes produce a subtle bruit, especially during Valsalva (holding breath or straining) (pmc.ncbi.nlm.nih.gov) (pmc.ncbi.nlm.nih.gov).
Finally, and often most importantly, the affected eye shows elevated intraocular pressure (IOP). As the episodes of venous hypertension progress, the IOP may climb significantly (we have seen cases over 30 mmHg) (pmc.ncbi.nlm.nih.gov) (pmc.ncbi.nlm.nih.gov). Ophthalmologists will notice an engorged episcleral venous plexus on exam, often with blood visible in Schlemm’s canal (the eye’s drainage channel). A standard applanation tonometry test may even show “wobbly” blinking tonometer mires reflecting the pulsatility of the eye. In one report, more than 64% of patients with CCF had high IOP (22–55 mmHg) (pmc.ncbi.nlm.nih.gov). In short, a swollen, red, pulsating eye with corkscrew vessels and a bruit should immediately raise concern for a fistula (pmc.ncbi.nlm.nih.gov) (pmc.ncbi.nlm.nih.gov).
Imaging the Fistula and Eyes
If a CCF is suspected from the eye exam, imaging is the next step. Several tests can pick up clues:
- CT or MR Angiography: These non-invasive scans of brain vessels can show an enlarged cavernous sinus, a dilated superior ophthalmic vein, or early filling of the venous system. They often suggest a fistula and can guide planning (pmc.ncbi.nlm.nih.gov) (pmc.ncbi.nlm.nih.gov).
- Ultrasound with Doppler: A skilled sonographer can sometimes detect reversed blood flow in an orbital vein or a “color bruit” of turbulent flow. Eye ultrasound may show an enlarged or pulsating ophthalmic vein.
- Gadolinium-enhanced MRI/MRA: Can reveal enlargement and abnormal flow voids in the orbit and cavernous sinus.
However, the gold standard for diagnosis and exact classification is digital subtraction catheter angiography (DSA) (pmc.ncbi.nlm.nih.gov) (pmc.ncbi.nlm.nih.gov). This is an invasive X-ray test where contrast dye is injected into the carotid and other arteries under fluoroscopy. Angiography precisely shows the location, size, and type of fistula, and whether it is draining anteriorly to the eye or posteriorly to the brain. For example, angiography will diagnose a Barrow type A vs. D fistula and show if the superior ophthalmic vein is filling backward. It also allows measurement of flow. In practice, ophthalmologists often first order a CTA or MRA if suspicious, then confirm with angiography (pmc.ncbi.nlm.nih.gov) (pmc.ncbi.nlm.nih.gov).
Endovascular Treatment and IOP Effects
Management of a CCF usually involves an interventional radiologist or neurosurgeon working with the eye doctor. The main goal is to occlude (block) the fistula, stopping the abnormal blood flow and restoring normal venous drainage.
- In direct (type A) fistulas, treatment is usually urgent. A catheter is threaded through the femoral or carotid artery to the cavernous sinus, and the connection is closed off with coils, balloons, or liquid embolic agents. Modern detachable balloons or platinum coils can seal the tear in the artery. Sometimes a stent or liquid glue (onyx) is used. Heidelberg et al. reported using a detachable balloon in a direct CCF (pmc.ncbi.nlm.nih.gov).
- In dural (indirect) fistulas (types B-D), the decision to treat depends on symptoms. Because these are low-flow, some will spontaneously close or remain asymptomatic. If eye pressure is high or vision is threatened, treatment is indicated (pmc.ncbi.nlm.nih.gov) (pmc.ncbi.nlm.nih.gov). The embolization may go through arterial feeders or, more commonly, a transvenous approach via the venous system (through the inferior petrosal sinus or rarely via a cutdown on the superior ophthalmic vein). The goal is to deliver coils or liquid to the cavernous sinus to plug the fistula from the vein side.
These endovascular procedures have become highly effective and relatively safe (pmc.ncbi.nlm.nih.gov). After the fistula is closed, venous pressure in the orbit drops and the eye congestion resolves. Notably, intraocular pressure often falls quickly. Case reports and series document dramatic IOP improvement after successful embolization (pmc.ncbi.nlm.nih.gov) (link.springer.com). For instance, in one case, IOP in one eye dropped from 34 mmHg to 19 mmHg just one week after CCF closure (pmc.ncbi.nlm.nih.gov). Another study found that embolization lowered the patient’s IOP by about 9 mmHg on average (link.springer.com). In that report, after angiographic occlusion of a bilateral CCF, both eyes’ pressures fell from the mid-20s into the high teens (link.springer.com). This confirms that fixing the fistula is often the most powerful way to reduce eye pressure.
Adjunct medical therapy for glaucoma is usually given until the fistula is closed. Patients may use combinations of eyedrops (beta-blockers, carbonic anhydrase inhibitors, prostaglandin analogs) and oral acetazolamide to help manage the pressure. However, high episcleral venous pressure often blunts the effect of drops. Once flow is normalized, the same medications become more effective at maintaining a normal pressure (pmc.ncbi.nlm.nih.gov) (pmc.ncbi.nlm.nih.gov).
If embolization fails or only partially succeeds and IOP remains dangerously high, eye surgery may be needed. Options include laser trabeculoplasty or filtering surgeries (trabeculectomy, shunts). Recent reports note that glaucoma drainage devices (tube shunts) can be life-saving: in one case of indirect CCF where embolization was incomplete, implanting an Ahmed valve finally normalized the pressure (pmc.ncbi.nlm.nih.gov). However, most experts attempt fistula closure first whenever possible, because that often solves the glaucoma root cause (link.springer.com) (pmc.ncbi.nlm.nih.gov).
Balancing Eye Treatment vs Fistula Closure
Deciding when to treat the eye pressure versus the fistula depends on urgency and feasibility. Generally, if the patient can safely wait a short time, the priority is to close the fistula, because doing so treats the underlying cause of high IOP. In one report, authors emphasized that transluminal occlusion of the fistula should be done before any glaucoma surgery (link.springer.com). After closure, they saw enough pressure drop that more invasive eye surgery was often avoided. Indeed, many cases show substantial IOP reduction immediately after successful embolization (pmc.ncbi.nlm.nih.gov) (link.springer.com).
However, if the eye pressure is extremely high or the patient has severe vision loss, simultaneous measures are needed. For example, if optic nerve damage is imminent, an ophthalmologist may place a drainage shunt or perform laser trabeculoplasty while planning the fistula embolization. Medications and even laser peripheral iridotomy can be performed to reduce IOP temporarily. In practice, doctors will manage the glaucoma medically as best they can until the fistula is closed. As Heichel et al. put it, closing the fistula should be considered before planning any glaucoma surgery (link.springer.com), whenever feasible.
Here are two illustrative cases:
-
Case 1: A 73-year-old woman had long-standing mild glaucoma, then developed new bulging eyes, double vision, and a red left eye. Her untreated IOP shot up above 30 mmHg. Imaging (MR angiography) found a direct CCF. After transarterial coil embolization of the fistula, her chemosis and proptosis largely resolved and IOP quickly fell into the teens on modest medication (pmc.ncbi.nlm.nih.gov). This case shows how closing the fistula normalized orbital pressure and improved glaucoma control.
-
Case 2: A 48-year-old woman presented with a red, proptotic eye and very high IOP in that eye (mid-40s), initially thought to be inflammation. Angiography revealed a dural (type D) CCF. Endovascular embolization achieved only near-complete closure. Although venous congestion improved, her eye pressure remained elevated despite drops. Further embolization attempts failed, so the team implanted an Ahmed glaucoma valve shunt in the affected eye. After the tube surgery, her IOP dropped into the normal range (pmc.ncbi.nlm.nih.gov). This example underscores that if embolization can’t fully fix the pressure issue, glaucoma surgery is the necessary backup.
In summary, most experts agree on a multidisciplinary approach (pmc.ncbi.nlm.nih.gov). Ophthalmologists should treat the eye to protect vision (drops, laser) while neuroradiologists or neurosurgeons plan embolization. When possible, the fistula is treated first, which often eases or cures the glaucoma. When fistula closure is difficult or delayed, targeted glaucoma surgery can stabilize the eye (pmc.ncbi.nlm.nih.gov).
Conclusion
Carotid-cavernous fistulas are an important and treatable cause of secondary glaucoma. By shunting high-pressure blood into the cavernous sinus, they raise orbital venous pressure and episcleral pressure, leading to eye redness, proptosis, and markedly elevated intraocular pressure (pmc.ncbi.nlm.nih.gov) (pmc.ncbi.nlm.nih.gov). Recognizing the signs – corkscrew conjunctival veins, chemosis, bruit, and a “pulsating” eye – is crucial for prompt diagnosis. Non-invasive imaging (CTA/MRA) followed by angiography confirms the diagnosis and guides treatment. Modern endovascular therapy (coils, balloons, etc.) can usually close the fistula safely (pmc.ncbi.nlm.nih.gov). Closing the fistula tends to normalize eye pressure, often dramatically reducing the need for aggressive glaucoma surgery (pmc.ncbi.nlm.nih.gov) (link.springer.com). Patients with CCF require close collaboration between eye doctors and neuro-interventionists, but with timely care the outlook is good – the ocular venous congestion can resolve and vision can often be preserved.
**`