Introduction
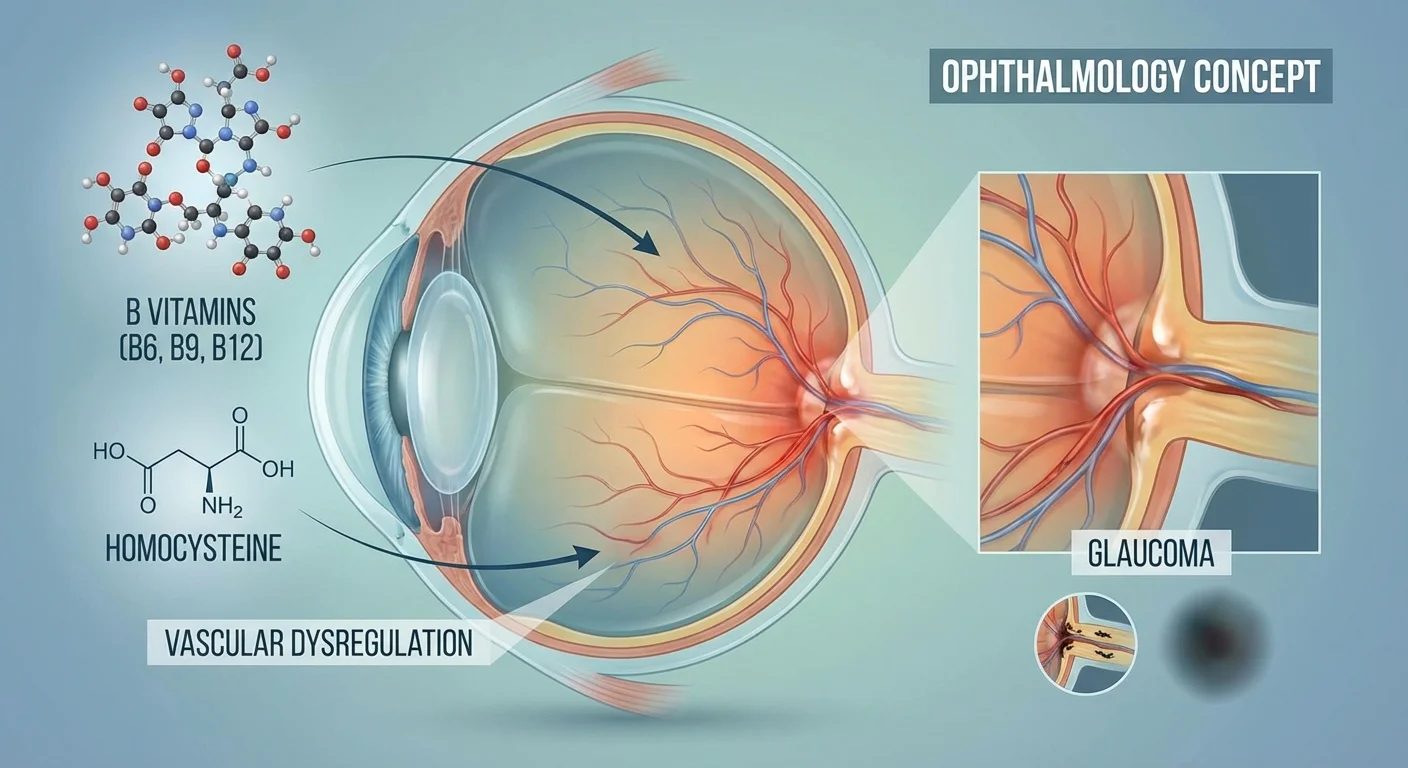
Glaucoma is an age-related optic neuropathy in which retinal ganglion cells and their fibers in the optic nerve gradually die, often silently, leading to vision loss. While high intraocular pressure is a well-known risk factor, blood vessel health also matters – poor blood flow or vascular dysregulation in the optic nerve head can contribute to glaucoma progression. Homocysteine (Hcy) is an amino acid metabolite that normally circulates at low levels (5–15 µmol/L) in the blood. When homocysteine rises (called hyperhomocysteinemia), it can injure endothelial cells (the inner lining of blood vessels) and promote oxidative stress and inflammation in the microvasculature (pmc.ncbi.nlm.nih.gov). This endothelial dysfunction is a recognized step toward atherosclerosis and cardiovascular disease, and it may plausibly stress the small blood vessels that nourish the optic nerve. In fact, studies have long noted that people with glaucoma – especially certain types – tend to have higher homocysteine and lower folate (vitamin B9) levels (pmc.ncbi.nlm.nih.gov) (pmc.ncbi.nlm.nih.gov). For example, in pseudoexfoliation glaucoma (a form of open-angle glaucoma), one study found significantly elevated homocysteine and correspondingly low folate; the authors concluded that “elevated levels of Hcy in [these patients] may explain the role of endothelial dysfunction” in that disease (pmc.ncbi.nlm.nih.gov) (pmc.ncbi.nlm.nih.gov). In short, elevated homocysteine is known to damage blood vessels through oxidative stress, inflammation, and impaired nitric oxide signaling, and this could translate into optic nerve microvascular stress in glaucoma (pmc.ncbi.nlm.nih.gov).
Homocysteine and Glaucoma
Research suggests that homocysteine-related vascular damage is relevant to glaucoma. For example, animal models of glaucoma show retinal metabolic disturbances long before nerve cell loss. In one recent study, normal (rodent) eyes exposed to intraocular pressure elevation had higher retinal homocysteine, and experimentally raising Hcy in the eye caused a small increase (≈6%) in ganglion cell death. Importantly, however, large genetic studies in humans (UK Biobank) found that having genetically higher homocysteine did not predict worse glaucoma outcomes (pmc.ncbi.nlm.nih.gov). This hints that high Hcy may be a pathogenic feature – a consequence or exacerbating factor – rather than a primary cause of glaucoma. Nonetheless, these animal models also showed that supplementing deficiencies in one-carbon metabolism (the biochemical pathways using B vitamins) can protect the nerve. Namely, giving a cocktail of vitamin B6, folic acid (B9), vitamin B12, and choline to glaucoma-model rodents prevented retinal ganglion cell loss and preserved visual function (pmc.ncbi.nlm.nih.gov). In short, high homocysteine appears to stress the optic nerve (especially in the context of metabolic or genetic defects), and B-vitamin–related pathways can counteract that stress.
B Vitamins and Homocysteine Reduction
Vitamins B6, B9 (folate), and B12 are essential co-factors in homocysteine metabolism—B9 and B12 help remethylate homocysteine back to methionine, and B6 helps convert homocysteine to cystathionine for breakdown. Giving these vitamins reliably lowers plasma homocysteine. Meta-analyses show that supplementing folic acid, B6 and B12 reduces homocysteine by roughly 25–30% over several years (pmc.ncbi.nlm.nih.gov). In one large review of trials (over 22,000 participants), B-vitamin therapy cut total homocysteine by about 26–28% but had no significant effect on cognitive test scores or global mental function (pmc.ncbi.nlm.nih.gov). In practical terms, lowering Hcy with B vitamins did not slow down cognitive aging in those trials (the difference in cognitive decline rate was effectively zero) (pmc.ncbi.nlm.nih.gov).
However, there is evidence that certain vascular outcomes can improve with B-vitamin therapy. Network meta-analyses of stroke-prevention trials found that regimens containing folic acid and vitamin B6 were most effective at reducing stroke risk. In a combined analysis of 17 trials (~86,000 patients), any B-vitamin supplementation modestly reduced the risk of stroke and brain hemorrhage. The best outcomes came with folic acid plus B6: this combination lowered stroke risk significantly compared to placebo, whereas combinations with B12 alone were less effective (pmc.ncbi.nlm.nih.gov). Similarly, the China Stroke Primary Prevention Trial (CSPPT) showed that in hypertensive adults, adding folic acid (0.8 mg) to blood-pressure therapy cut first-stroke risk by about 21% (hazard ratio 0.79) compared to blood-pressure therapy alone (pubmed.ncbi.nlm.nih.gov). This benefit was most pronounced in those with the common MTHFR “TT” genotype (a variant that impairs folate metabolism and raises homocysteine) and in a population without folic acid food fortification (pubmed.ncbi.nlm.nih.gov).
Notably, homocysteine-lowering may yield benefits especially in people with vascular risk factors or vitamin deficiencies. Where diets are low in folate (as in China before fortification), trials have found significant stroke risk reduction with folic acid (pubmed.ncbi.nlm.nih.gov). In contrast, many Western trials saw smaller or no effect, possibly because cereal grains are already fortified with folic acid. In any case, the vascular effects of B vitamins bring up an interesting parallel: if systemic vessel health improves, could the optic nerve’s microvasculature also benefit? No glaucoma trial has definitively answered this yet, but the brain/vascular data provide a rationale for studying it.
Effects on Cognitive Aging
Although homocysteine is linked to Alzheimer’s and cognitive decline in observational studies, high-quality trials have generally not shown cognitive benefit from B-vitamin therapy (pmc.ncbi.nlm.nih.gov). For example, the meta-analysis of 11 trials found that even though B vitamins robustly lowered Hcy, they did not improve memory, processing speed, or overall cognition in older adults (pmc.ncbi.nlm.nih.gov). A few smaller trials hinted at slowed brain atrophy in people with very high baseline Hcy, but these results have not yet translated into clear clinical guidelines. The bottom line is that, as of 2025, routine B-vitamin supplementation is not proven to prevent memory loss in generally healthy older adults (pmc.ncbi.nlm.nih.gov).
Homocysteine, Genetics, and Glaucoma Risk
Genetics can strongly influence homocysteine levels. A well-known example is the MTHFR C677T polymorphism: people with the “TT” genotype have a reduced-activity form of the MTHFR enzyme and tend to have higher homocysteine, especially if folate is low. In cardiovascular research, MTHFR variants have been associated with higher stroke and heart disease risk (particularly in low-folate settings) (pmc.ncbi.nlm.nih.gov). In the eye, things are still unclear. In mice genetically deficient in MTHFR, the retina accumulates homocysteine and shows increased retinal ganglion cell death, suggesting that MTHFR dysfunction could raise glaucoma risk via elevated Hcy (pmc.ncbi.nlm.nih.gov). However, human studies of MTHFR polymorphisms and glaucoma have yielded mixed results. Some meta-analyses hint at a slight association in certain populations, but others find no clear link (pmc.ncbi.nlm.nih.gov). In practice, knowing someone’s MTHFR type might help identify those who “run high” on homocysteine, especially if their diet is poor in B vitamins. For such individuals (or those with known B vitamin deficiencies), targeted supplementation (for example, using L-methylfolate instead of folic acid) could be considered.
Safety of B Vitamin Supplementation
Vitamins B6, B9, and B12 are generally safe when taken at recommended doses. Standard daily supplements (e.g. B6 1–2 mg, B12 2–3 mcg, folic acid 400–800 mcg) are well within nutritional guidelines. Higher doses can have issues: for example, vitamin B6 in doses above ~100–200 mg per day can cause peripheral neuropathy over time, and excessive folic acid (above ~1000 mcg/day) can mask a B12 deficiency, potentially delaying diagnosis of a serious condition. Vitamin B12 has no established upper limit and is water-soluble (excess is excreted), even in high doses. Some observational studies raised concerns about very high-dose B-vitamin supplements and cancer risk (notably lung cancer in smokers), but clinical trials have shown mixed results on this. Overall, moderate B-vitamin use appears safe, and any serious side effects are rare. There is no evidence that these vitamins harm the eyes; in fact, some ophthalmologists use B-vitamins for other eye conditions (e.g. B12 for optic neuropathy) without harm. As always, supplements should be considered in the context of the individual patient: for example, checking that high-dose folate is not given to someone with undiagnosed B12 deficiency.
Future Directions: Ophthalmic Trial Endpoints
To date, most research on homocysteine and B vitamins has focused on heart, brain, and stroke outcomes – not eye diseases. No large clinical trial has specifically tested whether lowering homocysteine (via diet, supplements, or medication) slows glaucoma onset or progression. Given the safety of B vitamins and their ability to lower Hcy, it would be valuable for future glaucoma studies to include ophthalmic endpoints. For example, a trial of folate (or combined B6/B12/folate) in adults with early glaucoma could measure changes in optic nerve imaging (OCT), visual field progression, or ocular blood flow. Such endpoints would directly test whether homocysteine-lowering translates into eye benefits. It would also be useful to screen glaucoma patients for hyperhomocysteinemia or MTHFR variants, to see if those subgroups derive greater benefit. Until then, any connection between homocysteine and glaucoma remains an interesting hypothesis supported by biology and indirect evidence, but not by direct clinical proof.
Conclusion
Elevated homocysteine can damage tiny blood vessels and trigger endothelial dysfunction, processes implicated in glaucomatous optic neuropathy. Epidemiological and animal studies suggest high Hcy and low folate/B12 may contribute to optic nerve stress, while B-vitamin supplementation can reduce Hcy and even protect retinal neurons in models (pmc.ncbi.nlm.nih.gov) (pmc.ncbi.nlm.nih.gov). In humans, trials have shown that B6, B12 and folate appreciably lower Hcy, but effects on disease outcomes have been mixed: cognitive decline was not slowed (pmc.ncbi.nlm.nih.gov), whereas stroke risk was modestly reduced (pmc.ncbi.nlm.nih.gov) (pubmed.ncbi.nlm.nih.gov). The analogy to glaucoma is still speculative. In the broader aging literature, homocysteine-lowering is not clinically recommended except in specific high-risk scenarios, yet the idea of improving microvascular health with vitamins is appealing. Given the emerging data, it would be prudent to avoid vitamin B deficiencies in glaucoma patients and to consider targeted supplements in those with known hyperhomocysteinemia or MTHFR risk. Ultimately, well-designed trials with glaucoma-specific endpoints are needed to answer whether B-vitamin strategies can help protect vision as we age.